New Jersey’s main cash assistance program for families has lost more than a third of its buying power since 1998.[1] A family of three now qualifies for a maximum of $559 a month, barely enough to cover the cost of groceries for most of the month, let alone rent, utilities, or transportation.[2] This is Temporary Assistance for Needy Families (TANF), the program designed to help families through hard times.
The program reaches fewer families than it once did. This does not mean poverty has fallen. Instead, it shows that TANF has become too difficult to access for the families who need it most.
Families are better positioned to get through hard moments when they have economic stability. But when someone loses a job, faces a medical crisis, or struggles to make ends meet, too many families lack the resources that would prevent a short-term setback from becoming a long-term hardship. That burden falls hardest on low-income families, which is why cash assistance is an effective tool the state uses to lift families out of poverty. New Jersey should strengthen TANF, so families count on support when hard times hit.
This explainer answers common questions about how TANF works, who it serves, what is at stake for New Jersey families, and how the state can improve it.
What is TANF?
Temporary Assistance for Needy Families (TANF) is a federal poverty-fighting program that provides states with a fixed annual amount of money to support cash assistance — or monthly payments — and work-related services for low-income families.[3] Congress created TANF in 1996 to replace the prior government assistance system, Aid to Families with Dependent Children (AFDC), and to give states broad flexibility in designing and running their own programs.[4] To receive funding year after year, states contribute their own state dollars, called Maintenance-of-Effort, and adhere to federal TANF’s guidelines.[5]
At its core, TANF is meant to be a bridge: time-limited support that keeps families afloat during moments of financial crisis while they work toward long-term stability through employment, education, or securing stable housing.[6] However, from the beginning, the program was shaped more by the goal of moving people off government assistance than by a commitment to eliminating poverty.[7] That early design framework, rooted in outdated and racialized assumptions about who needs help and how to deliver it, has survived for nearly three decades.[8] Reforming New Jersey’s TANF program is an opportunity to correct those longstanding shortcomings and bring it in line with today’s economic realities, ensuring it functions as the vital tool families have always needed.
How Does TANF Connect to Work First New Jersey (WFNJ)?
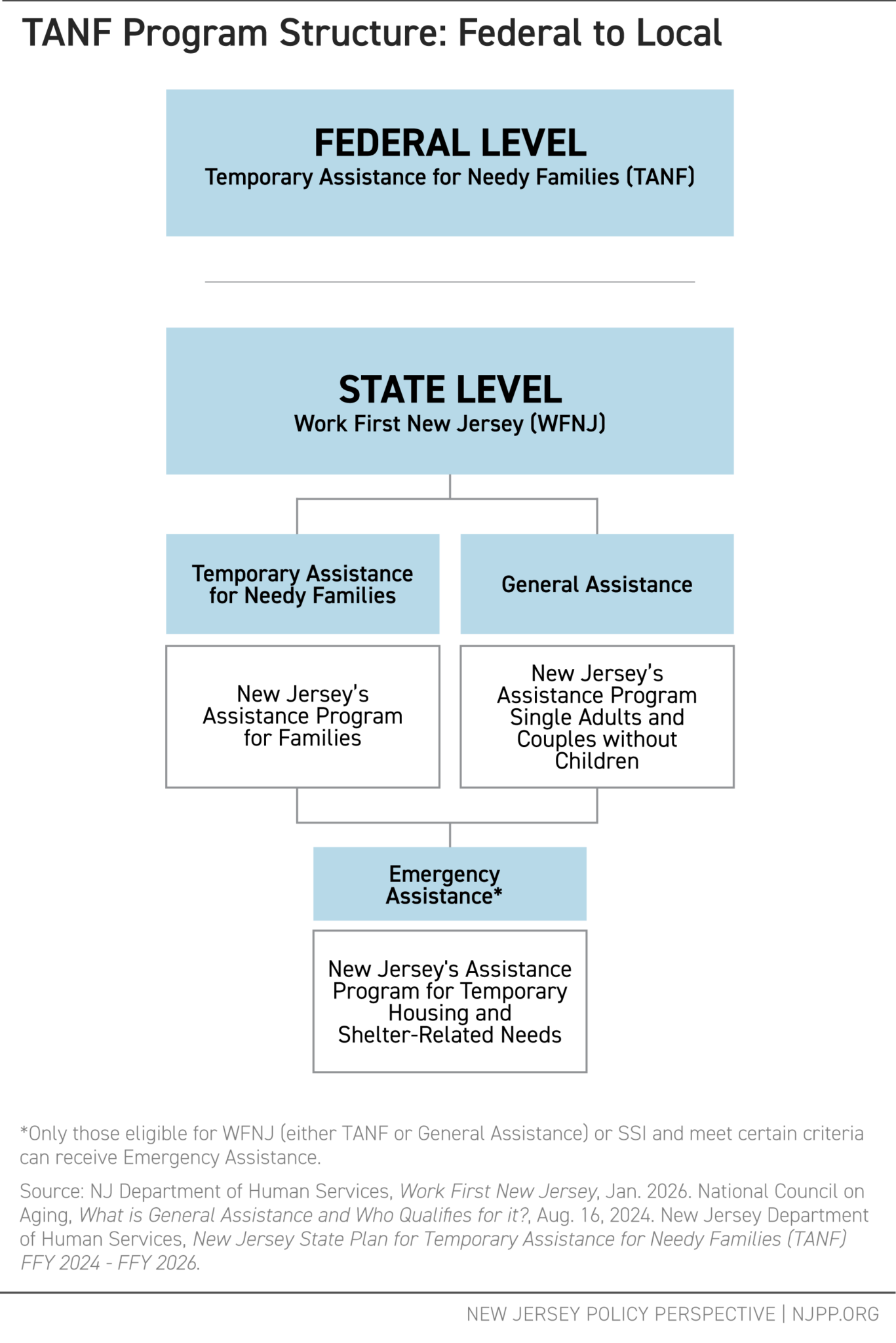
In New Jersey, the federal Temporary Assistance for Needy Families program is administered through Work First New Jersey (WFNJ), an umbrella program run by the state Department of Human Services’ Division of Family Development that oversees several work-related programs.[9] WFNJ was created in response to a federal “welfare overhaul,” known as the Personal Responsibility and Work Opportunity Reconciliation Act of 1996, and provides temporary cash assistance, work supports, and employment services to eligible residents.[10]
The WFNJ program has three main parts:
- Temporary Assistance for Needy Families (TANF): Cash assistance and work supports for families with dependent children and low incomes.[11]
- General Assistance (GA): A state-funded program for single adults and childless couples who are not eligible for TANF.[12] New Jersey is one of only a few states that still offer this benefit.[13]
- Emergency Assistance (EA): Short-term housing and shelter-related help available to people who qualify for WFNJ and meet certain requirements.[14]
Who Qualifies for TANF in New Jersey?
Families with dependent children (children up to age 18) can get TANF cash assistance if they meet strict income and asset requirements. However, the eligibility rules have not been updated in any major way since 1997, even as the cost of living has climbed in the state.[15]
To qualify and keep benefits, families must follow these rules:
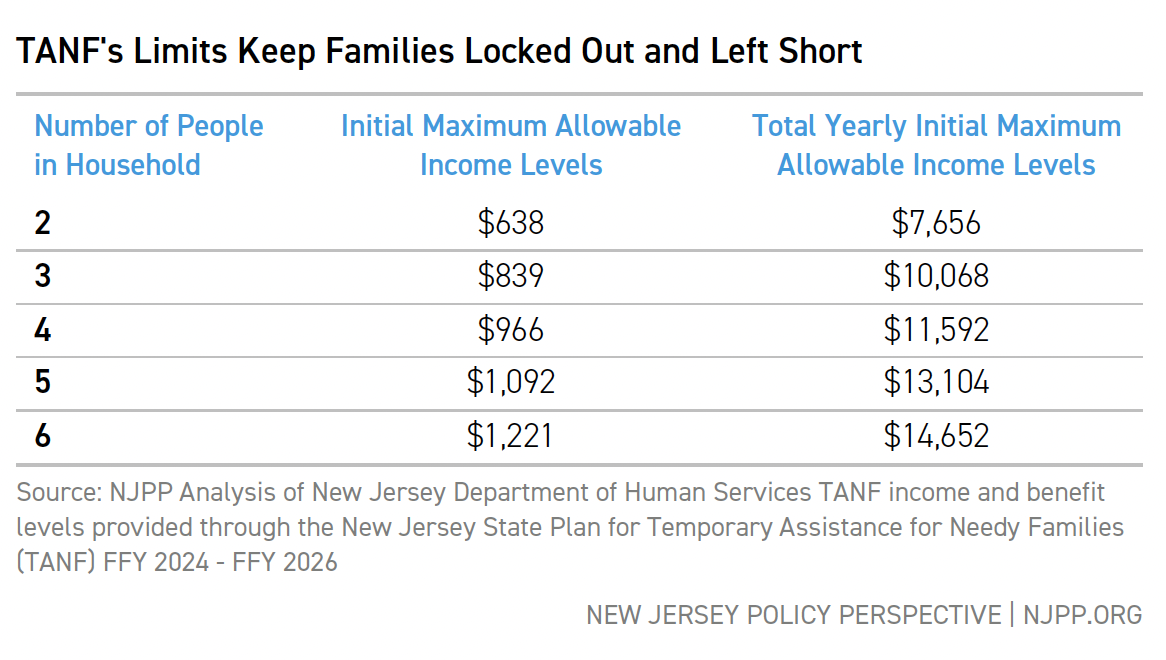
Financial eligibility and limitations
- Monthly income below a specific amount based on family size.[16]
- Families can keep no more than $2,000 in resources (for example savings in a bank account), except for specific exempt resources (examples of exemptions are ownership of a motor vehicle or property that does not produce revenue).[17]
- All income is counted when determining eligibility (for example a portion of child support or dividend earnings), except for specific exempt sources (examples of exemptions are income tax refunds and SSI benefits).[18]
Work and participation requirements
- Parents must participate in work activities for at least 35 hours each week.[19]
- A specific set of educational or vocational activities may count toward meeting work activity requirements for a period of time.[20]
Time limits and family rules
- Cash assistance is limited to five years (60 months) over a lifetime, with the exception of families that qualify for New Jersey’s extreme hardship category.[21]
- Work activities must begin within the first two years (24 months) of receiving assistance.[22]
- Non-compliance can result in a full-family penalty, or withholding of assistance, though it is not imposed immediately.[23]
Administrative and other requirements
- Parents must cooperate with child support rules. This includes giving the state rights to child support payments, with only a small amount of those payments passed on to families with children.[24]
- Most non-citizen or lawful permanent residents are not allowed to receive assistance during their first five years in the United States, though exemptions exist for groups such as refugees, people seeking asylum, and others with specific protections.[25]
Why Are the Eligibility Rules so Strict?
TANF’s harsh features are not the product of neutral policymaking. They were shaped by racialized narratives about poverty that dominated federal cash assistance debates from the 1960s through the 1990s. These stories painted certain parents, Black mothers in particular, as irresponsible and unwilling to work. Policymakers then used those stereotypes to justify tying assistance to behavioral requirements.[26]
New Jersey went further than federal law required on many of these restrictions. The Garden State was the first in the nation to adopt a family cap policy, which denied additional assistance to parents who had another child while receiving TANF.[27] The policy rested on the deeply racist assumption that Black and Brown people were having children irresponsibly or to increase their benefits.[28] In reality, it carried forward a legacy of reproductive control and punishment, treating family growth as something to be regulated rather than a basic human right, and ignoring the causes of poverty in favor of policing parents’ decisions.[29]
Although New Jersey repealed the family cap in 2020, the underlying assumptions did not disappear.[30] The same stereotypes that feed into the idea of families needing to be monitored, corrected, or punished into “responsible” behavior continue to shape many of TANF’s current rules, including work requirements that go further than federal law and other policies that make it harder for families to enter, remain in, or exit the program.[31]
How Much Do Families Actually Receive?
Families receive very little compared to the cost of living. For a family of three, the maximum monthly cash payment is $559 (about $6.13 per person per day), but many families receive less than the maximum.[32] On an annual basis, the maximum benefit for a family of that size is $6,708.[33] For context, a family of three spends more than $10,000 a year on food alone in New Jersey.[34] The 2026 federal poverty level for a family of three is $27,320, meaning that the maximum TANF grant amounts to less than a quarter of that figure.[35]
Benefit levels have also lost significant ground to inflation. As of 2026, the TANF grant has lost more than 34 percent of its buying power since 1998.[36] The most meaningful increase to the benefit level came in 2019-2020, when the maximum grant was last increased.[37] While that increase helped, it only partially restored what two decades of inflation had worn away; the grant has continued to fall behind New Jersey’s rapidly rising housing, food, and transportation costs ever since.
To better illustrate the decline in buying power, consider the following: the 1998 TANF payment for a family of three was $424, but in 2026 dollars it is equal to $853.38.[38] Today’s grant stands at $559, a few hundred dollars less, and has been fixed for more than seven years.[39] If a family was relying on the monthly TANF maximum grant in years 1998 and 2026, and spending simply on some of the recommended dietary food items in the USDA Thrifty Food Plan, here’s what grocery costs would look like:

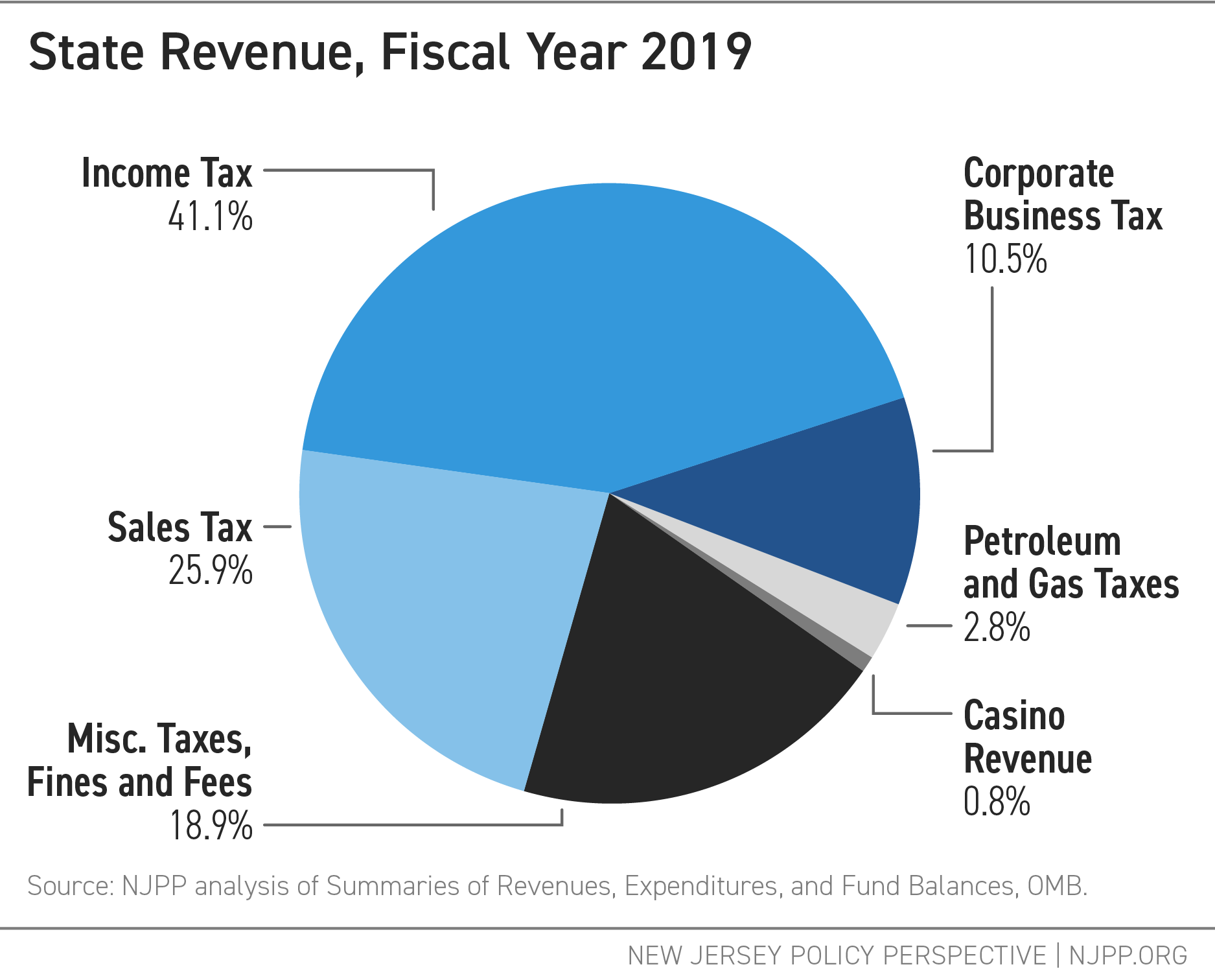
How is TANF Funded?
TANF is funded through a mix of federal and state dollars. The federal government provides New Jersey with a fixed annual amount of nearly $403 million in Fiscal Year 2023.[40] That amount has not changed since 1996, meaning its real value has eroded significantly over nearly 30 years. This also means that the funding has not accounted for inflation, shifts in populations, or changes in those eligible for or receiving assistance.[41]
To access those federal funds, New Jersey must also contribute state money through a requirement known as Maintenance-of-Effort (MOE).[42] MOE rules require states to spend a minimum amount of non‑federal money based on what they invested in pre‑TANF programs in Fiscal Year 1994.[43] For New Jersey, this means maintaining spending at either 80 percent or 75 percent of its 1994 level.[44] The threshold varies depending on two factors:
- whether the state meets its federal work participation rate, and
- whether the state provides funding to tribal TANF programs operating within its borders.
New Jersey does not have a tribal TANF program because there are no federally recognized tribes in the state.[45] However, it must still meet federal work participation standards — 50 percent of all families and 90 percent of families with two parents must be engaged in qualifying work activities.[46] In federal Fiscal Year 2024, the state’s MOE spending in TANF and separate programs totaled just more than $1.67 billion.[47]
Within these broad requirements, states have considerable flexibility in how they use TANF dollars.[48] Funds can support monthly payments, pre‑K programs, job training, and cover a wide range of expenses such as “transportation, child care, or other costs necessary for participating, such as uniforms, books, or supplies.”[49]
In New Jersey, however, only about five percent of TANF funds go toward direct cash assistance, specifically in the form of monthly grants, for families in crisis.[50] A much larger share is directed toward other programs, including pre-K and refundable tax credits.[51] While this flexibility is valuable, it also means that little TANF funding reaches families in the form of monthly grants when they need it most.
Is TANF Being Threatened by Federal Cuts?
Since early 2025, the federal government has been considering significant cuts to the federal TANF program.[52] Because TANF has fixed annual funding, any federal cut would directly reduce the resources available to states. States would then face difficult choices: reduce benefits and services, or use state funds to make up the difference.
At the same time, the federal government has threatened cuts or already disrupted several other core safety net programs such as the Low Income Home Energy Assistance Program, the Supplemental Nutrition Assistance Program (SNAP), and other programs that many TANF-receiving families rely on to meet basic needs.[53] Instability across these programs, combined with delays in federal funding, risks worsening conditions for New Jersey’s underserved families at a moment when the safety net is already stretched thin.
Has TANF Been Effective at Reducing Poverty?
TANF’s monthly grants remain one of the most important tools New Jersey has to lift families out of poverty. Cash assistance has consistently been shown to work: when families receive direct income support, they experience greater stability, children have better health and educational outcomes, and parents are better able to build long‑term economic security.[54] But these benefits only materialize when programs are adequately funded, accessible, and designed to meet real need.
As it is now, TANF reaches too few families with too little cash support. In the nearly three decades since the 1996 welfare reform, the program has grown increasingly difficult to access, even as the need has not gone away.
A few numbers show how much ground has been lost:
- The program reaches far fewer families than it once did. Before TANF replaced AFDC, New Jersey assisted well above the national average of 72 per 100 families in poverty.[55] In 2022-2023, New Jersey served only 11 families per 100, far below the national average of 20.[56]
- Enrollment is dangerously low, but the need is not. In 2025, TANF served an average of 26,500 people across New Jersey's 21 counties, a sharp drop from nearly 31,300 the previous year.[57]
- Children have borne the brunt of TANF’s decline. TANF’s decline has eliminated monthly payments to thousands of children statewide, from 163,997 children in 1997 to 20,446 children in 2024, with the steepest count losses in high-poverty counties like Camden, Essex, and Hudson.[58] This is a stark contrast to the reality that one in nine children in New Jersey experiences poverty.[59]
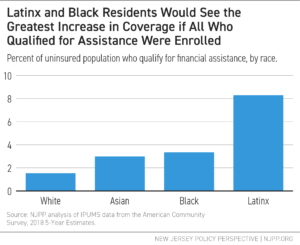
The gap between what TANF could do and what it currently does is felt most by Black and Hispanic/Latinx families, who in Fiscal Year 2023 made up 47.8 percent and 31.9 percent of NJ TANF recipients, respectively.[60] These disparities reflect long-standing racial inequities in income, employment, and wealth — inequities that shape who most needs support from a program like TANF. They also reveal who is too often left without help because of the program’s restrictive design and limited reach, especially in communities that have been historically excluded from economic opportunity.[61] The answer is not to abandon TANF. It is to make it work the way it is supposed to.
What Reforms Are Needed?
Efforts to reform TANF have been ongoing in New Jersey for years.[62] Some important changes have already been secured, including a one-time grant increase in state fiscal year 2020 and the repeal of the family cap policy.[63] But broader reform has remained out of reach. A comprehensive bill addressing a wider range of TANF shortcomings has moved through the statehouse year after year without passing.
The proposals below reflect the core areas where reform advocates and legislators have focused their efforts, and where New Jersey must act to build a stronger, more modern TANF:
- Raise benefit levels and keep them up with inflation. The most urgent change is increasing the monthly grant amount. The current 2026 maximum benefit covers only a fraction of what it costs to live in New Jersey.[64] The monthly payment should be raised to at least 50 percent of the federal poverty level and New Jersey should adopt an automatic cost‑of‑living adjustment so that grants keep pace with inflation without requiring annual legislative action.[65]
- Direct more money to cash assistance. New Jersey currently allocates only about five percent of its TANF block grant toward direct cash assistance.[66] That share should be much higher. Prioritizing TANF dollars in the form of monthly grants, rather than diverting them to other programs, would ensure that funds reach families who need immediate support to pay rent, buy food, and cover basic expenses.
- Update eligibility rules and time limits. Eligibility rules must be modernized so families enter, remain in, and transition off TANF more smoothly. This includes:
- Raising income and asset limits to reflect today’s costs.[67]
- Simplifying applications and reducing documentation requirements.[68]
- Addressing chronic administrative understaffing to improve access.[69]
- Aligning work requirements with reality. New Jersey’s work requirements exceed federal standards, requiring 35 hours each week for most parents. This is often impossible for families dealing with unstable jobs, irregular schedules, limited child care, or health challenges.[70] Aligning state rules with federal guidelines would reduce unnecessary case closures and better reflect the realities of low‑wage work. Just as important, TANF should treat a broader range of education, training, and earning credentials as core work activities. Recognizing these pathways as fully valid would support long‑term economic progress rather than punishing families for circumstances beyond their control.
- Fix the benefits cliff. Under current rules, even a modest increase in earnings may trigger a sudden loss of benefits, hurting stability.[71] Expanding the amount of earnings that do not count against benefits would allow families to keep more support as savings as their wages grow. This would give parents the breathing room to build financial stability gradually rather than face an abrupt cutoff the moment their income rises.
Conclusion
Strengthening TANF is one of the most direct ways the state can lift families out of poverty. But doing that requires confronting decades of policy choices that have steadily narrowed who has access to help and how much they receive.
State lawmakers have a critical role to play. By raising benefit levels, updating outdated eligibility rules, and redirecting more TANF money toward the families the program was built to serve, New Jersey can build a safety net that meets families where they are. With a stronger TANF, the state can reduce deep poverty by ensuring families in crisis have a floor to stand on.
End Notes
[1] NJPP Analysis of U.S. Department of Health and Human Services Federal 2026 Poverty Guidelines to determine the amounts for varying federal poverty levels, Work First New Jersey grant amounts provided through the New Jersey state budget and Department of Human Services, and Bureau of Labor Statistics Consumer Price Index Calculator to consider inflation, Jan. 2026.
[2] New Jersey Department of Human Services, New Jersey State Plan for Temporary Assistance for Needy Families (TANF) FFY 2024 - FFY 2026, Schedule I and Schedule II, 2024.
[3] Congressional Research Service, The Temporary Assistance for Needy Families (TANF) Block Grant: A Legislative History, Jan. 6, 2025.
[4] Center on Budget and Policy Priorities, Policy Basics: Temporary Assistance for Needy Families, Mar. 1, 2022.
[5] Congressional Research Service, Temporary Assistance for Needy Families (TANF) Block Grant: A Primer, Aug. 26, 2025. Lower-Basch, E. and Burnside, A., TANF 101: Block Grant, The Center for Law and Social Policy, Mar. 2025.
[6] Congressional Research Service, The Temporary Assistance for Needy Families (TANF) Block Grant: A Legislative History, Jan. 6, 2025.
[7] Lower-Basch, E. and Burnside, A., TANF 101: Block Grant, The Center for Law and Social Policy, Mar. 2025.
[8] Floyd, Ife, et al., TANF Policies Reflect Racist Legacy of Cash Assistance, Center on Budget and Policy Priorities, Aug. 4, 2021.
[9] Note that the state’s TANF program is often referred to as WFNJ/TANF or simply TANF.
[10] Justia Regulations, NJ Admin Code 10:90-1.1, Jun. 16, 2025. Floyd, Ife, et al., TANF Policies Reflect Racist Legacy of Cash Assistance, Center on Budget and Policy Priorities, Aug. 4, 2021.
[11] NJ Department of Human Services, Work First New Jersey, Jan. 2026.
[12] NJ Department of Human Services, Work First New Jersey, Jan. 2026.
[13] National Council on Aging, What is General Assistance and Who Qualifies for it?, Aug. 16, 2024. Schott, L., General Assistance Programs Very Limited in Half the States and Nonexistent in Others, Despite Need, Center on State on Budget and Policy Priorities, Jul. 22, 2020.
[14] People who receive Supplemental Security Income (SSI), which provides monthly payments to individuals with limited income and resources, including those who are 65 or older, blind, or disabled, are also eligible to apply for emergency assistance. See for example: New Jersey Department of Human Services, New Jersey State Plan for Temporary Assistance for Needy Families (TANF) FFY 2024 - FFY 2026. Social Security Administration, Supplemental Security Income (SSI) in New Jersey, 2026.
[15] New Jersey’s TANF program has seen some changes throughout the years, but these changes were too specific and limited in nature. See for example: Center on Budget and Policy Priorities, States Should Follow New Jersey: Repeal Racist “Family Cap”, Oct. 14, 2020. Department of Human Services, Murphy Administration Boosts Payments for Families & Individuals in Need, Sep. 4, 2019.
[16] New Jersey Department of Human Services, New Jersey State Plan for Temporary Assistance for Needy Families (TANF) FFY 2024 - FFY 2026, Schedule I, 2024.
[17] NJ Department of Human Services, Get Work First New Jersey, Jan. 2026.
[18] New Jersey Department of Human Services, New Jersey State Plan for Temporary Assistance for Needy Families (TANF) FFY 2024 - FFY 2026, pg. 21, 2024.
[19] New Jersey Department of Human Services, New Jersey State Plan for Temporary Assistance for Needy Families (TANF) FFY 2024 - FFY 2026, pg. 24, 2024.
[20] New Jersey Department of Human Services, New Jersey State Plan for Temporary Assistance for Needy Families (TANF) FFY 2024 - FFY 2026, pg. 29, 2024.
[21] States are allowed to extend families’ support beyond the lifetime limit if they fall under certain state-defined categories of “extreme hardship.” Those categories can include serious medical conditions, domestic violence situations, and more. However, states can only provide this exemption of the lifetime limit and extension of support for up to 20 percent of their caseload. Families that qualify for New Jersey’s 20 percent extreme hardship category are supported through a separate program funded with state money. New Jersey Department of Human Services, New Jersey State Plan for Temporary Assistance for Needy Families (TANF) FFY 2024 - FFY 2026, pg. 12, 19, and 24, 2024.
[22] New Jersey Department of Human Services, New Jersey State Plan for Temporary Assistance for Needy Families (TANF) FFY 2024 - FFY 2026, pg. 24, 2024.
[23] NJ Department of Human Services, Staying on Work First New Jersey, Jan. 2026.
[24] NJ Department of Human Services, Get Work First New Jersey, Jan. 2026.
[25] New Jersey Department of Human Services, New Jersey State Plan for Temporary Assistance for Needy Families (TANF) FFY 2024 - FFY 2026, pg. 15, 2024.
[26] Floyd, Ife, et al., TANF Policies Reflect Racist Legacy of Cash Assistance, Center on Budget and Policy Priorities, Aug. 4, 2021. Floyd, I., States Should Follow New Jersey: Repeal Racist “Family Cap”, Center on Budget and Policy Priorities, Oct. 14, 2020.
[27] Covert, B., New Jersey, Birthplace of Welfare Family Caps, Has Finally Repealed Them, TalkPoverty, Oct. 16, 2020.
[28] Floyd, I., States Should Follow New Jersey: Repeal Racist “Family Cap”, Center on Budget and Policy Priorities, Oct. 14, 2020.
[29] Patel, U. and Shrivastava, A., Reproductive Justice and TANF: Repealing “Family Cap” Policies Promotes Economic Justice and Family Autonomy, Center on Budget and Policy Priorities, Dec. 19, 2023.
[30] Covert, B., New Jersey, Birthplace of Welfare Family Caps, Has Finally Repealed Them, TalkPoverty, Oct. 16, 2020.
[31] Floyd, I., States Should Follow New Jersey: Repeal Racist “Family Cap”, Center on Budget and Policy Priorities, Oct. 14, 2020. Floyd, Ife, et al., TANF Policies Reflect Racist Legacy of Cash Assistance, Center on Budget and Policy Priorities, Aug. 4, 2021. Patel, U. and Shrivastava, A., Reproductive Justice and TANF: Repealing “Family Cap” Policies Promotes Economic Justice and Family Autonomy, Center on Budget and Policy Priorities, Dec. 19, 2023. New Jersey Department of Human Services, New Jersey State Plan for Temporary Assistance for Needy Families (TANF) FFY 2024 - FFY 2026, pg. 24, 2024.
[32] New Jersey Department of Human Services, New Jersey State Plan for Temporary Assistance for Needy Families (TANF) FFY 2024 - FFY 2026, Schedule I and Schedule II, 2024. State of New Jersey, The Governor’s FY 2027 Budget: Detailed Budget, pg. D-244 - pg. D-245, Mar. 2026.
[33] NJPP Analysis of New Jersey Department of Human Services, New Jersey State Plan for Temporary Assistance for Needy Families (TANF) FFY 2024 - FFY 2026, Schedule I and Schedule II, 2024.
[34] Massachusetts Institute of Technology, Living Wage Calculation for New Jersey, Feb. 28, 2026.
[35] NJPP Analysis of U.S. Department of Health and Human Services Poverty Guidelines for 2026 to determine the amounts for varying federal poverty levels, Jan. 2026.
[36] NJPP Analysis of U.S. Department of Health and Human Services Federal Poverty Guidelines for 2026 to determine the amounts for varying federal poverty levels, Work First New Jersey grant amounts provided through the New Jersey state budget and Department of Human Services, and Bureau of Labor Statistics Consumer Price Index Calculator to consider inflation, Jan. 2026.
[37] Department of Human Services, Murphy Administration Boosts Payments for Families & Individuals in Need, Sep. 4, 2019. Holom-Trundy, B., Adjusting Work First New Jersey Eligibility Would Help Tackle Child Poverty, New Jersey Policy Perspective, Feb. 14, 2022. Holom-Trundy, B., Expand Anti-Poverty Programs to Help Families in Crisis, New Jersey Policy Perspective, Jan. 22, 2025.
[38] NJPP Analysis of New Jersey Department of Human Services New Jersey State Plan for Temporary Assistance for Needy Families (TANF) FFY 2024 - FFY 2026 of grant amounts on Schedule II and Bureau of Labor Statistics Consumer Price Index Calculator to consider inflation, Jan. 2026.
[39] Department of Human Services, Murphy Administration Boosts Payments for Families & Individuals in Need, Sep. 4, 2019
[40] Center on Budget and Policy Priorities, New Jersey TANF Spending, Jan. 16, 2026.
[41] Congressional Research Service, Temporary Assistance for Needy Families (TANF) Block Grant: A Primer, Aug. 26, 2025. Congressional Research Service, The Temporary Assistance for Needy Families (TANF) Block Grant: A Legislative History, Jan. 6, 2025.
[42] Congressional Research Service, Temporary Assistance for Needy Families (TANF) Block Grant: A Primer, Aug. 26, 2025.
[43] Administration for Children & Families, Categories and Definitions for TANF and MOE Funds, Nov. 13, 2020. Congressional Research Service, Temporary Assistance for Needy Families (TANF) Block Grant: A Primer, Aug. 26, 2025.
[44] Congressional Research Service, Temporary Assistance for Needy Families (TANF) Block Grant: A Primer, Aug. 26, 2025.
[45] Administration for Children & Families, Help for Families: TANF Program Contact Information, Accessed Mar. 23, 2026.
[46] Congressional Research Service, Temporary Assistance for Needy Families (TANF) Block Grant: A Primer, Aug. 26, 2025.
[47] Administration for Children & Families, TANF Financial Data - FY 2024, Jan. 22, 2026.
[48] Congressional Research Service, Temporary Assistance for Needy Families (TANF) Block Grant: A Primer, Aug. 26, 2025. Congressional Research Service, The Temporary Assistance for Needy Families (TANF) Block Grant: A Legislative History, Jan. 6, 2025.
[49] NJ Department of Human Services, Get Work First New Jersey, Jan. 2026.
[50] Center on Budget and Policy Priorities, New Jersey TANF Spending, Jan. 16, 2026.
[51] Administration for Children & Families, TANF and MOE Spending and Transfers by Activity, FY 2024: New Jersey, Nov. 21, 2025.
[52] Luhby, T., Trump is freezing funds for small but key welfare program. Here’s what TANF does, CNN, Jan. 7, 2026. Schmit, S. and Wilensky, R., Cuts to SSBG, TANF Would Eliminate Child Care for 40K Children, Disrupt Care for Millions More, The Center for Law and Social Policy, Mar. 2026,
[53] Macartney, S. and Ghertner, R., How Many People that Receive One Safety Net Benefit Also Receive Others?, U.S. Department of Health and Human Services, Jan. 20, 2024. Lucas, A. and Repko, M., Proposed SNAP cuts could pressure low-income shoppers — and retailers that serve them, CNBC, Apr. 16, 2025. Harvard Kennedy School, Explainer: Understanding the SNAP program—and what cuts to these benefits may mean, Nov. 10, 2025. Picchi, A. and Cunningham, M., Low-income families face a financial cliff as government shutdown threatens 4 federal aid programs, CBS News, Oct. 31, 2025.
[54] Haider, Areeba, et al., Re-Envisioning TANF: Toward an Anti Racist Program That Meaningfully Serves Families, Georgetown Center on Poverty and Inequality, Oct. 20, 2022.
[55] Center on Budget and Policy Priorities, Trends in State TANF-to-Poverty Ratios, Oct. 1, 2025.
[56] Center on Budget and Policy Priorities, Trends in State TANF-to-Poverty Ratios, Oct. 1, 2025.
[57] NJ Department of Human Services, Current Program Statistics - December 2025, Table 1, Mar. 2026.
[58] NJPP analysis of ACNJ 1998 Kids Count data and DFD 2024 Current Program Statistics data, all years are for enrollment in June. Small Area Income and Poverty Estimates (SAIPE) data for poverty under age 18 for years 1997 and 2024.
[59] U.S. Census Bureau, Poverty Status in the Past 12 Months, American Community Survey, ACS 1-Year Estimates Subject Tables, Table S1701, Sep. 2024.
[60] Administration for Children & Families, Characteristics and Financial Circumstances of TANF Recipients, Fiscal Year 2023, Table 10, Oct. 3, 2024.
[61] Aguas, T., Census 2024: Economic Gains Bypass Many New Jersey Communities, New Jersey Policy Perspective, Oct. 21, 2025.
[62] Symons, M., Major overhaul of NJ’s welfare program passed by Senate, NJ 101.5, Apr. 14, 2020. Koball, H. and Hartig, S., Op-Ed: NJ’s TANF program falls short in supporting families in poverty, NJ Spotlight News, May 31, 2022. Castro, R., Promoting Equal Opportunities for Children Living in Poverty, New Jersey Policy Perspective, Apr. 2020.
[63] Department of Human Services, Murphy Administration Boosts Payments for Families & Individuals in Need, Sep. 4, 2019. Covert, B., New Jersey, Birthplace of Welfare Family Caps, Has Finally Repealed Them, TalkPoverty, Oct. 16, 2020.
[64] NJPP Analysis of TANF benefit amounts and 2026 federal poverty levels. See for example: U.S. Department of Health and Human Services Poverty Guidelines for 2026 to determine the amounts for varying federal poverty levels, Jan. 2026. New Jersey Department of Human Services, New Jersey State Plan for Temporary Assistance for Needy Families (TANF) FFY 2024 - FFY 2026, Schedule I and Schedule II, 2024.
[65] Azevedo-McCaffrey, D. and Aguas, T., Continued Increases in TANF Benefit Levels Are Critical to Helping Families Meet Their Needs and Thrive, Center on Budget and Policy Priorities, Feb. 26, 2025. Castro, R., Promoting Equal Opportunities for Children Living in Poverty, New Jersey Policy Perspective, Apr. 2020.
[66] Center on Budget and Policy Priorities, New Jersey TANF Spending, Jan. 16, 2026.
[67] Burnside, A. and Fairbanks, J, Eliminating Asset Limits: Creating Savings for Families and State Government, The Center for Law and Social Policy, Oct. 2023.
[68] There is no recent published research examining New Jersey TANF participants’ experiences with WorkFirst NJ specifically. However, studies from other states offer insight into how participation rules and administrative processes can shape families’ ability to remain on the program. Qualitative research from Illinois documents that many TANF recipients experience the program as difficult to navigate, with complex work requirements and procedural hurdles contributing to case closures. While these findings do not describe New Jersey’s system, they illustrate broader patterns in how TANF’s design can create barriers for families. See for example: Heartland Alliance, Resigned to the Process: Barriers to Accessing and Maintaining TANF among Low-Income Families with Young Children in Illinois, 2022.
[69] Holom-Trundy, B., Outdated and Ineffective: Why New Jersey Needs to Update Its Top Anti-Poverty Program, New Jersey Policy Perspective, May 22, 2025.
[70] There is no recent published research examining New Jersey TANF participants’ experiences with WorkFirst NJ specifically. However, studies from other states offer insight into how participation rules and administrative processes can shape families’ ability to remain on the program. Qualitative research from Illinois documents that many TANF recipients experience the program as difficult to navigate, with complex work requirements and procedural hurdles contributing to case closures. While these findings do not describe New Jersey’s system, they illustrate broader patterns in how TANF’s design can create barriers for families. See for example: Heartland Alliance, Resigned to the Process: Barriers to Accessing and Maintaining TANF among Low-Income Families with Young Children in Illinois, 2022.
[71] Stevens, W., Mitigating TANF Benefits Cliffs, National Conference of State Legislature, Mar. 1, 2024.