Their jobs do not offer health insurance, and their paychecks leave little room for premiums. Medicaid expansion closed this gap, providing quality coverage to residents working hard to get by.
Progress Is Now Threatened by Federal Cuts
Despite these improvements, residents living on low incomes and immigrants continue to face barriers to affordable health insurance. Now, federal lawmakers are withdrawing support from programs that serve families with the fewest resources, threatening to leave even more people without coverage.[29]
The ACA’s success shows that policy solutions work when properly funded and implemented. State leaders must build on this progress by countering federal cuts with state action.
State Leaders Must Counter Federal Cuts
New Jersey leaders must continue to adequately fund existing programs like Cover All Kids and take these additional actions to protect residents from federal cuts:
Expand State Subsidies on the GetCovered NJ Marketplace
The elimination of the protections provided during the COVID-19 pandemic — including enhanced premium tax credits on the health insurance marketplaces and fewer administrative barriers for continuous coverage — has set health coverage back in direct contradiction to the lessons learned during that crisis.[30]
By expanding state subsidies — the New Jersey Health Plan Savings — already provided through GetCovered NJ, the gaps created by federal cuts can be filled with a reliable funding source, ensuring that residents can continue to afford plans through the marketplace.[31] In recent years, the state spent $215 million in funds raised through a state assessment paid by health insurance companies on these subsidies to help lower the cost of plans for residents. Dedicating more state funds toward these subsidies can help to fill some of the gap left by the expected loss of $500 million in federal assistance.[32]
Improve Data Sharing and Enrollment Systems to Prevent Paperwork-Driven Coverage Loss
Beginning in 2027, adult Medicaid enrollees aged 19 to 64 will be required to complete 80 hours of “community engagement,” defined as qualifying work or community service unless enrolled in certain educational programs. If they do not meet the requirement and do not qualify for an exemption, they will lose coverage.[33] Additionally, many of those same enrollees — those adults enrolled through the ACA Medicaid expansion — will now be required to submit redetermination paperwork every 6 months, rather than once a year.[34] Both of these requirements increase the likelihood that people will lose coverage simply due to administrative barriers.[35]
The state must take immediate action to invest in cross-departmental data sharing to reduce the paperwork required of residents with low incomes to receive all of the support for which they are eligible. Additionally, improving the accessibility of programs dealing with enrollment and reporting in order to ensure that the paperwork is as easy to understand, fill out, and submit as possible will help to reduce the number of people who struggle to complete the requirements.[36] The recent massive coverage losses during the Medicaid unwinding — when the state had to reevaluate all Medicaid enrollees’ eligibility as pandemic protections were removed — emphasized the communication gaps and paperwork system barriers that residents face to maintain coverage.[37] Improvements to these systems are critical for protecting New Jerseyans.[38]
Establish a State Government-Backed Insurance Plan to Close Coverage Gaps
When people cannot afford health insurance, they go without coverage to pay rent, keep the lights on, and put food on the table.[39] Without immediate health concerns, these needs feel more urgent. No one should face this choice, yet it is the reality for many New Jerseyans because gaps in coverage options define the state's health care system.
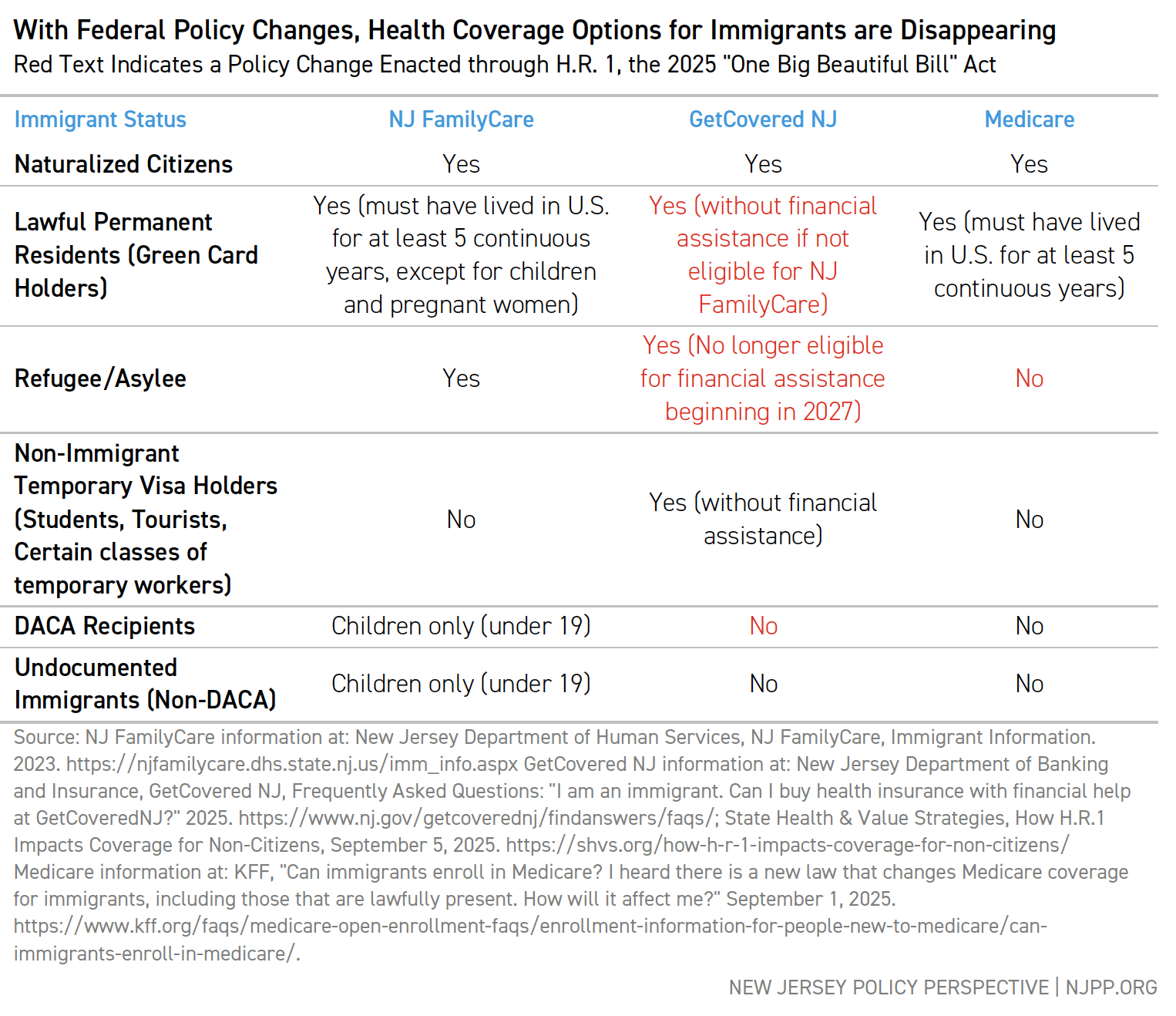
Currently, every affordable coverage option in the state, except NJ FamilyCare for children, limits eligibility based on immigration status or other factors. Many people cannot even buy into Medicaid, CHIP, or marketplace coverage by paying a reasonable premium — they are simply shut out.
State leaders should establish a government-backed health insurance plan — a “public option” — open to all residents regardless of age or immigration status. This would provide affordable coverage to residents who have limited or no options in the current system. A well-designed public option can also reduce costs system-wide and improve affordability for everyone.[40]
Ensure Equal Access to Enrollment Across Counties
County social services boards help residents enroll in coverage, but their staffing and outreach vary widely.[41] In counties where leaders refuse to commit resources, fewer eligible residents get enrolled.
The state should strengthen oversight of county boards and require better pay and benefits to attract qualified staff. These steps would reduce gaps between counties and help more New Jerseyans get covered.
Adequate staffing allows county workers to conduct targeted outreach to communities that face the highest barriers to enrollment, including immigrant communities that need language assistance and trust-building efforts.[42] This is especially true when exclusionary policies threaten immigrant communities more broadly.[43] When counties lack resources, these critical outreach efforts simply do not happen.
Conclusion
New Jersey has made remarkable progress expanding health coverage over the past decade. The Affordable Care Act brought insurance to more than half a million residents who previously went without. GetCovered NJ and Medicaid expansion closed critical gaps in the system.
Federal cuts now threaten to reverse this progress. Enhanced subsidies have expired, new work requirements will create paperwork barriers, and immigrants are losing access to affordable options. Without state action, thousands more New Jerseyans will lose coverage.
State leaders have the power to protect residents and their families. By increasing state subsidies, fixing broken enrollment systems, creating a public option, and ensuring equal county access to enrollment support, New Jersey can counter federal cuts and continue expanding coverage to those who need it most.
The choice is clear: act now to protect New Jerseyans, or watch a decade of progress disappear.
The stakes are clear. Will state leaders act to protect residents, or will they allow federal cuts to strip coverage from hundreds of thousands of working families?
End Notes
[1] U.S. Census Bureau, American Community Survey -- 2024 1-Year Estimates, Table S2701, 2025. The 1-year estimate, rather than the 5-year estimate, is provided here to give the most current picture of the number of uninsured in light of the significant changes that have happened through the Medicaid unwinding and other point-in-time effects.
[2] For a full timeline of the federal cuts affecting New Jersey, see: Ambrose, A., Chen, P., Holom-Trundy, B., and Ubel, M., State Lawmakers Should Protect Residents from Federal Cuts to Vital Services, New Jersey Policy Perspective, Aug. 2025.
[3] McGough, M., State-Based Efforts Will Provide Limited Relief from Enhanced Tax Credit Expiration, KFF, Jan. 2026. New Jersey Department of Banking and Insurance, Impact of Proposed Congressional Reconciliation Bill Package on New Jersey Residents Enrolled in Health Coverage Through Get Covered New Jersey, Jun. 2025.
[4] New Jersey Department of Human Services, Statement from Human Services Commissioner Sarah Adelman, Jul. 2025.
[5] Holom-Trundy, B., Beyond the Pandemic: New Data Reveals Growing Health Insurance Coverage Gaps, New Jersey Policy Perspective, Sep. 2024. Buettgens, M., et al., 4.8 Million People Will Lose Coverage in 2026 If Enhanced Premium Tax Credits Expire, Urban Institute, Sep. 2025. Lo, J., et al., ACA Marketplace Premium Payments Would More than Double on Average Next Year if Enhanced Premium Tax Credits Expire, KFF, Sep. 2025.
[6] McGough, M., State-Based Efforts Will Provide Limited Relief from Enhanced Tax Credit Expiration, KFF, Jan. 2026.; New Jersey Department of Banking and Insurance, DOBI Response to OLS Questions on FY 2026 Budget, Jun. 2025. Biryukov, N., Rates on NJ health insurance marketplace to skyrocket, state regulator warns, New Jersey Monitor, Oct. 2025.
[7] Centers for Medicare & Medicaid Services, Bulletin on Section 71119 of the “Working Families Tax Cut” Legislation, Public Law 119-21: Requirements for States to Establish Medicaid Community Engagement Requirements for Certain Individuals, Dec. 2025.
[8] Sommers, B.D., Goldman, A.L., Blendon, R.J., Orav, J., and Epstein, A.M., Medicaid Work Requirements — Results from the First Year in Arkansas, The New England Journal of Medicine, v. 381, no. 11, Jun. 2019. Medicaid and CHIP Payment and Access Commission (MACPAC), An Updated Look at Rates of Churn and Continuous Coverage in Medicaid and CHIP, Oct. 2021.
[9] KFF, Health Provisions in the 2025 Federal Budget Reconciliation Bill, Jul. 2025.
[10] New Jersey Department of Human Services, Stay Covered NJ Renewal Data, Jun. 2024.
[11] Stainton, L., Thousands of legal immigrants in NJ could be thrown off Medicaid, NJ Spotlight News, Jul. 2025.
[12] For eligibility limitations, see the NJ FamilyCare website: New Jersey Department of Human Services, NJ FamilyCare - Who is Eligible? and NJ Familycare - Immigrant Information, 2025. For the estimate of the loss due to recent federal changes, see: New Jersey Department of Human Services, Statement from Human Services Commissioner Sarah Adelman on Impact of Medicaid and SNAP Cuts on NJ, Jul. 2025. Imperato, N. and Doobay, K., Evaluating the Policy Implications and Impact of Health Insurance Literacy Initiatives, New Jersey State Policy Lab, Rutgers University, 2025.
[13] National Conference of State Legislatures, COVID-19: Essential Workers in the States, Jan. 2021.
[14] NJPP Analysis of U.S. Census Bureau, American Community Survey – 2024 5-Year Estimates, Tables S2701 and S2702, 2025.
[15] Holom-Trundy, B., Unprecedented and Unequal: Racial Inequities in the COVID-19 Pandemic, New Jersey Policy Perspective, Oct. 2020. Ndugga, N., Pillai, D., Hill, L., & Artiga, S., Race, Inequality, and Health, In Altman, Drew (Editor), Health Policy 101, KFF, Oct. 2025. Philbin, M., et al. State-Level Immigration and Immigrant-Focused Policies as Drivers of Latino Health Disparities in the United States, Social Science & Medicine, v. 199, pp. 29-38, 2018.
[16] Yearby, R., Clark, B., and Figueroa, J.F., Structural Racism in Historical and Modern US Health Care Policy, Health Affairs, Feb. 2022.
[17] Holom-Trundy, B., Unprecedented and Unequal: Racial Inequities in the COVID-19 Pandemic, New Jersey Policy Perspective, Oct. 2020.
[18] NJPP Analysis of U.S. Census Bureau, American Community Survey -- 2024 5-Year Estimates, Table S2701, 2025.
[19] Clemente, I., and Casau, A., Covering All Kids: Strategies to Connect Children of Undocumented Status to Health Care Coverage, Center for Health Care Strategies, Feb. 2023.
[20] Novak, N.L., Kline, N., LeBrón, A.M.W., Lopez, W., Michelen, M., De Trinidad Young, M-E., Mitigating The Health Impacts Of Exclusionary Immigration Policies: An Evidence Review, Health Affairs Health Policy Brief, Nov. 2025.
[21] NJPP Analysis of U.S. Census Bureau, American Community Survey -- 2024 5-Year Estimates, Table 2701, 2025.
[22] Telesford, I., Winger, A., and Rae, M., Beyond Cost, What Barriers to Health Care do Consumers Face?, Peterson-KFF Health System Tracker, Aug. 2024.
[23] NJPP Analysis of U.S. Census Bureau, American Community Survey – 2010-2024 1-Year Estimates, Table S2701, 2025. The 1-year estimates were used for this comparison because the purpose was to compare two single points in time rather than an overall trend.
[24] New Jersey Department of Banking and Insurance, GetCovered NJ, 2025.
[25] KFF, Marketplace Enrollment, 2014-2025, 2025. Note that "marketplace" here refers to New Jersey's enrollment through the federally-run marketplace on HealthCare.Gov from 2014-2020 and then to the state-based marketplace, GetCovered NJ, from 2021 to today. New Jersey passed legislation in 2019 to create the state-based marketplace. See Office of Governor Phil Murphy, Governor Murphy Announces Launch of New State-Based Health Insurance Marketplace, Get Covered New Jersey, Oct. 2020. Holom-Trundy, B., GetCoveredNJ: How New Jersey’s State-Based Exchange Will Make Health Coverage More Affordable, New Jersey Policy Perspective, Nov. 2020.
[26] NJPP Analysis of KFF, Marketplace Enrollment, 2014-2025, 2025.The 2026 enrollment period is currently underway at the time of writing; it is on track to have enrollment numbers even higher than 2025. However, more enrollees are choosing lower level plans due to cost. See GetCovered NJ’s 2026 Open Enrollment Update, Week 9 Snapshot.
[27] NJPP Analysis of New Jersey Office of Management and Budget, Governor's FY 2026 Budget, Detailed Budget, p. D-209, Mar. 2025. Note that only the category "Expansion Childless Adults" is included here because some parents were covered through NJ FamilyCare prior to the Affordable Care Act's Medicaid expansion.
[28] N.J.A.C. 10:74-1.4, see definition of "NJ FamilyCare Alternative Benefit Plan (ABP)." U.S. Department of Health and Human Services, 2026 Poverty Guidelines: 48 Contiguous States (all states except Alaska and Hawaii), 2026.
[29] KFF, Health Provisions in the 2025 Federal Budget Reconciliation Law, Aug. 2025. Ambrose, A., Chen, P., Holom-Trundy, B., and Ubel, M., State Lawmakers Should Protect Residents from Federal Cuts to Vital Services, New Jersey Policy Perspective, Aug. 2025.
[30] Holom-Trundy, B., Beyond the Pandemic: New Data Reveals Growing Health Insurance Coverage Gaps, New Jersey Policy Perspective, Sep. 2024. Buettgens, M., et al., 4.8 Million People Will Lose Coverage in 2026 If Enhanced Premium Tax Credits Expire, Urban Institute, Sep. 2025. Lo, J., et al., ACA Marketplace Premium Payments Would More than Double on Average Next Year if Enhanced Premium Tax Credits Expire, KFF, Sep. 2025.
[31] New Jersey Department of Banking and Insurance, Lower Your Monthly Premiums with the NJ Health Plan Savings, GetCovered NJ, 2025.
[32] New Jersey Department of Banking and Insurance, DOBI Response to OLS Questions on FY 2026 Budget, Jun. 2025. Biryukov, N., Rates on NJ health insurance marketplace to skyrocket, state regulator warns, New Jersey Monitor, Oct. 2025.
[33] Centers for Medicare & Medicaid Services, Bulletin on Section 71119 of the “Working Families Tax Cut” Legislation, Public Law 119-21: Requirements for States to Establish Medicaid Community Engagement Requirements for Certain Individuals, Dec. 2025.
[34] KFF, Health Provisions in the 2025 Federal Budget Reconciliation Bill, Jul. 2025.
[35] Sommers, B.D., Goldman, A.L., Blendon, R.J., Orav, J., and Epstein, A.M., Medicaid Work Requirements — Results from the First Year in Arkansas, The New England Journal of Medicine, v. 381, no. 11, Jun. 2019. Medicaid and CHIP Payment and Access Commission (MACPAC), An Updated Look at Rates of Churn and Continuous Coverage in Medicaid and CHIP, Oct. 2021.
[36] Wagner, J., Singleton, S., and Stewart, M., A Guide to Reducing Coverage Losses Through Effective Implementation of Medicaid’s New Work Requirement, Center on Budget and Policy Priorities, Nov. 2025. Diana, A., et al., Challenges with Implementing Work Requirements: Findings from a Survey of State Medicaid Programs, KFF, Oct. 2025.
[37] New Jersey Department of Human Services, Stay Covered NJ Renewal Data, Jun. 2024.
[38] New Jersey Department of Human Services, Meeting of the Medical Assistance Advisory Council - January 2026 Presentation, Jan. 2026.
[39] While the approach to bills differ across individuals and families and their needs, people who are struggling to pay bills each month are more likely to say that they are worried about paying utilities, food, and rent than they are about paying for health coverage. As ability to pay for bills increases, the health care costs become the focus, demonstrating a shift in priorities and needs: Montero, A., Kearney, A., Valdes, I., Kirzinger, A., and Hamel, L., KFF Health Tracking Poll: Economic Views and Experiences of Adults Who Struggle Financially, KFF, Feb. 2024. Additionally, those who are uninsured are more likely to report challenges affording health care costs: Sparks, G., Lopes, L, Montero, A., Presiado, M., and Hamel, L., Americans’ Challenges with Health Care Costs, KFF, Dec. 2025. Most people who are uninsured report that they do not have coverage due to the high cost: See Figure 7 in Tolbert, J., Bell, C., Cervantes, S. and Singh, R., The Uninsured Population and Health Coverage. In Altman, D. (Editor), Health Policy 101, KFF, Oct. 2025.
[40] Monahan, C.H., Stovicek, N., and Giovannelli, J., State Public Option Plans Are Making Progress on Reducing Consumer Costs, To the Point (blog), The Commonwealth Fund, Nov. 2023. King, J. S., Gudiksen, K.L., and Brown, E.C., Are State Public Option Health Plans Worth It?, Harvard Journal on Legislation, v. 59, pp. 145-219, 2022.
[41] Holom-Trundy, B., Understaffed and Underfunded: Barriers to Effective Anti-Poverty Assistance, New Jersey Policy Perspective, Nov. 2024.
[42] Clemente, I., and Casau, A., Covering All Kids: Strategies to Connect Children of Undocumented Status to Health Care Coverage, Center for Health Care Strategies, Feb. 2023.
[43] Novak, N.L., Kline, N., LeBrón, A.M.W., Lopez, W., Michelen, M., De Trinidad Young, M-E., Mitigating The Health Impacts Of Exclusionary Immigration Policies: An Evidence Review, Health Affairs Health Policy Brief, Nov. 2025.